Edward Shorter is a social historian, professor at the University of Toronto, and well-known author of numerous books on the history of psychiatry. From Paralysis to Fatigue: A History of Psychosomatic Illness in the Modern Era is one of his earliest works.
Despite the disheartening title (suggested alternatives: “Somatization and its Discontents,” “Hysteresis in Hysteria: A History”), From Paralysis to Fatigue is an absorbing story about the changing face of psychosomatic illness in Europe and the U.S., bursting with quotes from letters, diaries, and medical conference proceedings from the past 300 years. It is also, somehow, a primer on predictive processing and memetics from 1992.
But wait - what exactly is psychosomatic illness? I should mention here that I’m a psychiatrist. Many people experience physical symptoms that aren’t the result of an identifiable medical condition. Instead, we attribute the cause to a mysterious process called somatization (when people are preoccupied with internal sensations like stomach pain, chest pain, back pain, dizziness, palpitations, nausea, fatigue, etc) or conversion disorder (when people have dramatic neurological symptoms like convulsions, paralysis, sudden blindness, inability to speak clearly, etc). This sort of thing is surprisingly common but not well understood. If pressed, most doctors would still explain it as “something something psychological factors” or throw up their hands altogether.
Shorter has a conceptual model for all of this, which he lays out in the introduction:
Our bodies send us the most disparate variety of signals about physical symptoms. Under some circumstances, we interpret these signals as evidence of disease, but the symptoms into which our minds cast this disease are just as determined by fashion as was the fashionable face of fin-de-siecle Vienna.
And:
People have always tried to achieve some kind of plausible interpretation of their physical sensations. They cast these sensations on the model of well-defined medical symptoms available in a kind of “symptom pool.”
This “symptom pool” metaphor sounds an awful lot like an analog formulation of predictive processing. There’s a bottom-up stream of formless sensory data, in this case consisting of interoception like “ascending colon just distended a little” or “left semicircular canals say our head is rotating.” There’s the top-down stream of predictions, here involving medical priors like “I have irritable bowel syndrome” or “a lot of my peers have been fainting lately.”
I think this model suggests that unexplained symptoms can arise in different ways. One person might have a bottom-up stream of internal sensation that’s unusually insistent, or a top-down stream with unusually imprecise health priors. They end up perpetually bothered by random pains, numbness and tingling that comes and goes, bloating and nausea, fatigue for no reason.
On the other hand, someone developing sudden paralysis, blindness, or convulsions seems to require a top-down process “predicting” that their body can no longer use a limb. It also requires that the idea of “sudden paralysis, blindness, or convulsions” is present as a concept or template - a meme - that’s plausible for the body to do.
The question is which symptoms are prominent in the meme pool at a given time, and how they got there. This is the story From Paralysis to Fatigue sets out to tell.
The narrative gets going around 1830. For many decades before this, Shorter asserts, “hysterical” patients presented with a wide assortment of unexplainable pains, numbness, vomiting, temporary blindness, fainting fits, and so on. These ailments often improved with neutral therapies like baths, enemas, and exorcisms, suggesting that, at least for some, the cause wasn’t an undiscovered medical disorder.
Reflex Theory
With the elucidation of spinal reflex arcs (the real thing - as in tapping your patellar tendon induces a brisk knee jerk) in the 1830s, Medicine happened upon a new organizing paradigm. Doctors knew that they could tap on one part of the body, some sort of signal traveled around, and another part of the body reacted. “It was a short step to an assertion that every organ in the body could reflexly influence every other organ. This was reflex theory.” So an irritated anus would affect gastric secretions and thereby cause indigestion, or stomach irritation could cause croup.
Reflex theory held sway for much of the 19th century. Patients and doctors found it “alluring” due to the patina of scientific legitimacy. Tendon reflexes are clearly observable and reliably reproduced. They’re even useful in diagnosing some disorders! It also, Shorter argues, primed patients and doctors to expect motor rather than sensory symptoms. Accepting the premise of bodily action at a distance, you can easily explain how disparate symptoms are all connected, “particularly in women because of the permanent state of irritability of the female pelvis.”
However much you thought that 19th century male doctors were obsessed with uteruses, I promise they were in fact more obsessed. There was a school of ophthalmologists in Breslau who studied the effect of uterine excitability on the eyes, “kopiopia hysteria:”
These patients are usually very garrulous and speak constantly of their pains, often in exaggerated terms…One patient had to close her eyes every time she went through a door, because otherwise the drafts caused her eye pain. Another patient said her eyes could not stand it if someone stood too close to her while speaking, a third said that reading gave her abdominal pain, a fourth claimed that after reading for a while the black letters started to seem green, the paper red, and so forth.
Gynecology was a new field at the time, and physicians eagerly applied new examination techniques and surgical procedures. Ironically, doctors of the era insisted it was the patients who fixated on their own reproductive organs. As you can imagine, this era included an atrociously high number of unnecessary hysterectomies, ovariectomies, and clitoridectomies, an upsetting trend Shorter covers in detail.
Speaking of upsetting.
Then there’s this:
In 1872 New York gynecologist Fordyce Barker described a thirty year-old married patient with a retroverted (backward-tilted) uterus who had taken to spitting at family members. ‘She had been suffering for three or four days with pain in the back and the head…excessively irritable and ill-tempered…[later that day] she began spitting at her mother [and to her husband] “not only spit in his face but violently seized his hair…’ Barker examined her vaginally and found the uterus firmly retroverted, ‘so that it required some force to replace it. As soon as this was done, she loudly ejaculated, and with a kind of satisfied grunt, ‘there now!’ at once ceased spitting, and became perfectly quiet and before I left the room she fell asleep.”
I’m 80% sure that Dr. Barker fabricated this whole case in a sort of Victorian medical equivalent of Letters to Penthouse.
Fits
Fits had always been a common psychosomatic symptom - convulsing, flinging limbs, writhing on the ground, speaking abnormally - the sort of thing traditionally called spirit or demon possession. Presumably, traditional folk medicine and exorcism worked by way of placebo, if that term even applies here. If the problem resolves, it’s an active treatment!
Anyway, in the 19th century West, fits came in two major categories: a “fainting trance” referred to as catalepsy, and the more dramatic convulsions. A representative sample from Connecticut, 1880s:
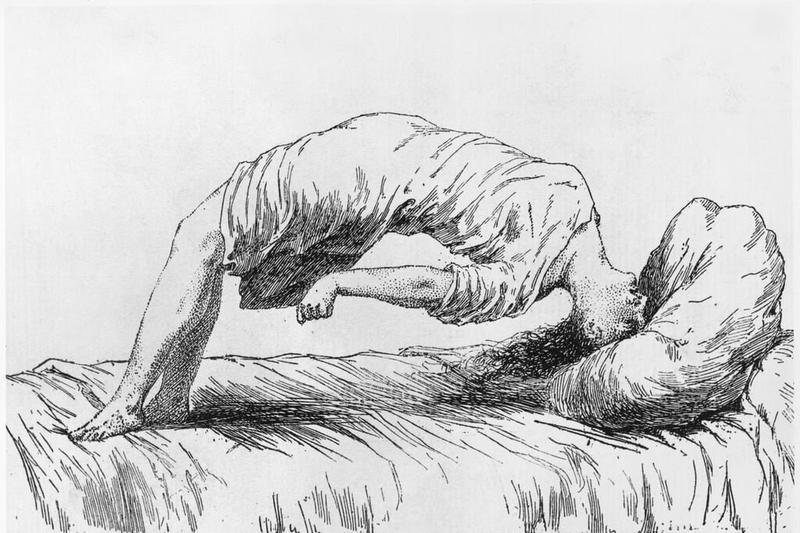
On a Sunday-school picnic a young lady was noticed by her friends to act queerly. She stopped talking, became absent-minded, stared about her in a dazed way, began to walk off…she soon began to get rigid and her face flushed. Then she commenced to go through various irregular movements of her body. She thrashed with her arms and kicked with her legs, threw her head from side to side, arched up her back and rolled about with such force that several of us had to hold her.”
Back arching as part of a fit. Looks a lot like opisthotonus in tetanus.
Neurologists and internists of the day built their practices managing such cases among the Victorian upper and middle classes.
Paralysis
“Hysterical paralysis” refers to sudden weakness, often in one or more limbs, that is not the result of an identifiable injury in the nervous system. In fact, there are findings on physical examination that are neurologically inconsistent, like a dragging gait (the person walks with their leg dragging behind) and the Hoover Test.
According to Shorter, this sort of complaint had been rare but exploded in the mid-19th century. Luckily, the usual treatment was not surgery but a stay at a spa. The book includes dozens of anecdotes involving a well-to-do woman who developed weakness, or inability to walk, or inability to speak, went to the seaside or a hot spring for several months, and then got better about half the time.
There was hysteria in men, too. A doctor in Munich saw a male lawyer in the 1840s:
The patient believed himself unable to move his toes, and was finally able to do so after I manipulated the joint a bit. Then he tried to walk, supported by someone on either side. That seemed to go well and I reassured him about the condition of his foot. Then because it was evening, I stayed a half hour to smoke a cigar with him. As I took my leave, he had forgotten his sick foot and accompanied me, lantern in hand, right to the stairs.”
Altered States
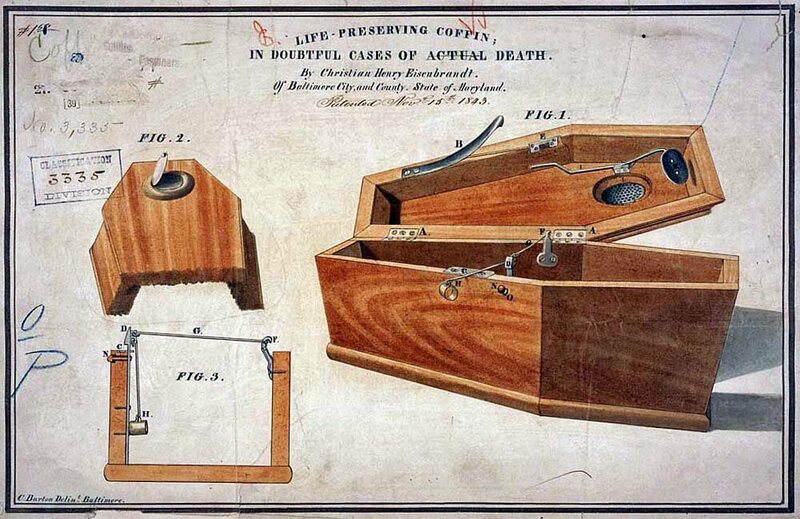
For several decades in the mid-1800s, a rage for “animal magnetism” and hypnosis swept Europe. It was basically classic stage hypnotism, in this case using magnets to make people hold contorted positions or say absurd things. It’s closely related to the idea of “second states,” “trance” or “catalepsy” mentioned above - people can spontaneously fall into unresponsive trance, apparently unconscious and unable to interact. Naturally, this led to a widespread fear of being buried alive and the advent of waiting mortuaries and safety coffins.
You’d be crazy NOT to buy one!
Awareness of hypnosis complicated psychosomatic presentations. People who might once have fallen into passive catalepsy or a convulsing fit now adopted “second states” that included quite a lot of activity, often bizarre:
A Dr. Petetin saw a married woman of nineteen who had been having fits and now seemed dead. Suddenly, before the eyes of her astonished parents, she arose and began singing. Next she began convulsing. Four men could scarcely hold her. Petetin plunged her into a cold bath, where she recovered. Petetin gave her a tobacco enema. She began singing again. After much furor, he discovered he could communicate with her by speaking not to her ears but to her stomach
Shorter comes through with a good point: “a climate of suggestion can elicit…fashionable mental symptoms as well.”
A brief aside - at least in humans, there’s pretty good evidence for “functional cognitive disorders.” Many older adults experience subjective impaired memory and other cognitive deficits, but then exhibit internal inconsistency when tested - they do better on cognitive tasks when distracted by other stimuli. There’s also subjective insomnia - a whole set of people convinced they barely sleep, but polysomnography findings don’t support this at all. Perhaps you know some individuals who, despite doing just fine academically and professionally, are convinced their concentration is terrible.
Peak Hysteria
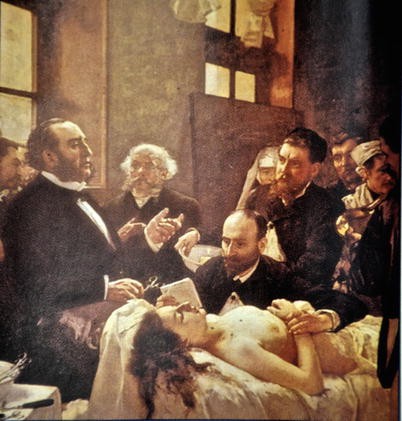
In the 1880s, at Salpetriere Hospital in Paris, the renowned neurologist Jean-Martin Charcot presided over an epidemic noteworthy even for the time. The cause seems to have been Charcot’s own baroque doctrine of hysteria, which postulated various phases (epileptiform convulsions, then large movements of the limbs and whole body, then delusions and hallucinations. These were further divided into tonic and clonic subphases, clownism, impassioned poses, a terminal period in which anything could happen. You get the idea.) Charcot loved putting on live demonstrations for younger physicians, creating an environment of drama and one-upmanship at the hospital.
A Clinical Lesson at the Salpetriere - this painting is famous.
Unsurprisingly, Charcot was obsessed with ovaries. In one demonstration he had his assistant press on a young woman’s left lower abdomen:
Immediately an attack of rhythmic chorea breaks out. The patient remains sitting and consciousness is reserved, her head begins suddenly to turn from right to left and then from left to right, in rhythmic alteration with equal pauses between the individual movements. Simultaneously the right arm begins going up and down, as a result of which her hand beats regularly on her knee as though on a drum…meanwhile the the right foot is stamping noisily on the floor
Charcot’s prestige was such that chic Parisian women briefly adopted similar behaviors as a kind of fashion. From a diary in 1889: “It is truly a bit unsettling…how society women are carrying on right now. They all seem like the hysteriques of the Salpetriere, let loose by Charcot upon the world.”
This whole episode is a clear example of the social contagion aspect of psychosomatic disorders: ideas and behaviors (memes) that spread via suggestion or imitation from person to person. In this particular case, the selection pressure came from Dr. Charcot and other physicians rewarding patients with attention and validation.
Predictably, such complex presentations dropped out of sight soon after Charcot’s death in 1893. Another famed neurologist, Dr. Babinski, looked back:
There was rarely a day when some patient was not in a hysterical crisis..and this was not just at the Salpetriere but in the other hospitals where similar scenes occurred…Today [la grande ataque] has virtually disappeared. It is no longer seen and other kinds of fits have become much rarer.
INTERLUDE
Tied with Document for third-best album of 1987.
Let’s take a step back. Isn’t this all kind of bizarre? Tons of people with blindness, paralysis, convulsions, trances, with no good explanation? And they aren’t even aware that “they” are doing it? OK, so wrong-headed medical paradigms, and sexism, and ubiquitous repression, and did I mention sexism, that’s all part of it. But why do humans even have the capacity to do this?
Because the ability to credibly feign illness and injury is super useful! Many bird species imitate a broken wing in order to distract predators from their nests. Dogs fake injured legs for food or sympathy, as do chimpanzees. If nothing else, this raises interesting questions about the theory of mind of shorebirds. The evolutionary logic applies to humans too: a convincing injury can evoke sympathy and aid from your tribe, signal submission to others, or get you out of dangerous tasks (“Yeah, I’d love to go on the mammoth hunt with you guys but…my leg is really acting up today.”)
But “convincing” is key, and Triver’s self-deception theory goes a long way here. Animals try to deceive each other all the time, and excel at spotting deception in others. Evolution’s best answer is for the animal itself to believe the deception, thereby avoiding the tell-tale signs of lying. In the case of psychosomatic illness, it means the symptom is produced unconsciously. A modern neuroscientist might say that the brain module producing the symptom is encapsulated, or inaccessible, to the speaking parts of your brain. The end result: symptoms that truly feel like the result of external influence.
So by the turn of the century fits, paralysis, and grand hysterical attacks were falling by the wayside. Shorter repeatedly emphasizes the class aspect - after several decades of high prevalence in the upper crust, paralysis and fits were passé, and by the interwar period appeared mostly in the working class.
Not coincidentally, a new medical paradigm was surpassing reflex theory. As scientists and physicians learned more about the brain in the late 1800s, medicine’s emphasis shifted to the idea that people could inherit “a kind of nervous constitution that affected their ‘cerebral centers.’” Soon cadres of “nerve doctors” trained as neurologists or internists sprung up in the bourgeois quarters of town across Europe and America.
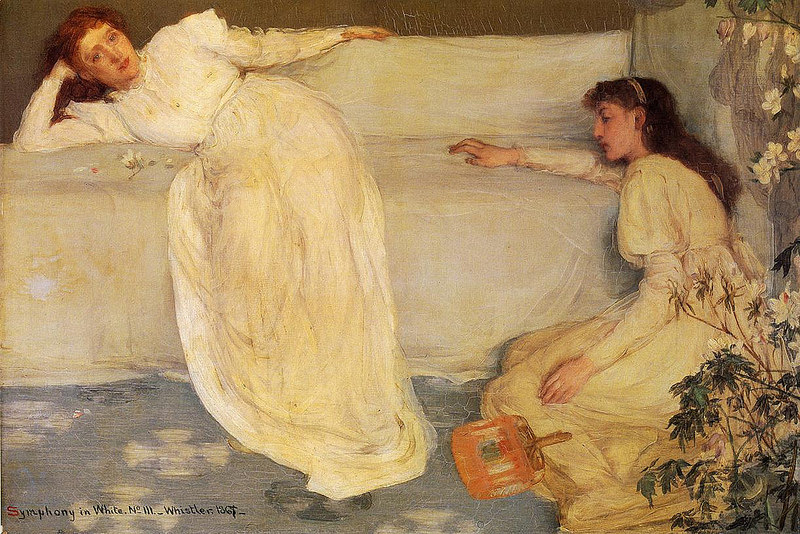
Edwardian lassitude.
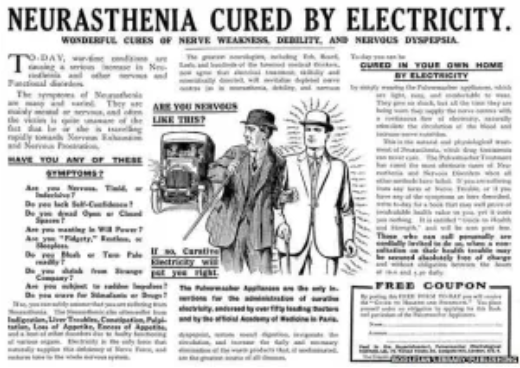
Neurasthenia
A new paradigm demanded a new label - neurasthenia. According to an observer in 1904, it “propagated like an epidemic. The name of neurasthenia is on everybody’s lips; and it is the fashionable new disease.” Here again, social contagion with a new illness meme - a memetic illness!
Neurasthenia was conceived of as an organic (i.e. real) nerve or brain condition that was partly heritable and partly due to stress. In practice, it functioned as a “grab-bag term for low-grade psychiatric symptoms.” A Dr. Drummond in Newcastle, 1907:
Anything between the highly strung, interesting, but irritable young lady who abhors the designation nervous, and is grossly insulted by the slightest hint she is hysterical when she complains of an abiding cold spot between her shoulders in her spinal column that nothing relieves, and the stupid, depressed, ever-complaining and, indeed, heartbreaking “lie-abed,” a lifelong trouble to herself and her friends; anything between the intelligent, vivacious business man with a fixed and altogether exaggerated idea of the importance of a certain sensation in his head or stomach, and the distressing state of neurotic impasse as represented by the lifelong depressed hypochondriac, we call neurasthenia, and their name is legion.
Neurasthenia, in contrast to the female identified hysteria, enabled nerve doctors to reach untapped markets: middle-class businessmen and the new urban working class.
Shorter highlights, over and over, that psychosomatic symptoms underwent a rapid change in character in a short time. Patients became “firmly fixated upon internal sensations in demonstration of the fact that they were ‘nervously ill.’ What a change this represented from a couple of decades earlier, when they were still convulsing, being paralyzed, and having limbs ‘draw up.’”
The neurasthenia brand soon diluted, though. By the 1920s it had “swollen to embrace virtually the entire range of psychic pathology, and thus had become meaningless.”
The Psychologization of Somatization
The story is complicated by the simultaneous emergence of a whole other paradigm emphasizing psychological factors.
This wasn’t just in Sigmund Freud’s circle. Respected neurologists, internists, and psychiatrists were soon referring to hysteria as a disease “of the subconscious mind, of unconscious suggestion.” Physicians argued to abolish the term hysteria and replace it with “psychogenic” illness. Eminent neurologist Adolf Strumpell wrote in 1893: “the number of apparently physical disorders which arise through primary psychological processes is at least as great as the number of actual organic disease conditions.”
This perspective, though surely an improvement on gynecologic surgery, had a major drawback. Physicians bought into the psychological paradigm and used it for the next century (and still do). But many patients hated it (and still do). Why? The psychological model for somatization implies that symptoms are separable into “organic” phenomena arising from the body and “psychological” phenomena arising from the mind. People aren’t dumb. This sounds a lot like some symptoms are legitimate, and others are in your mind - illegitimate.
Shorter sums up: “The psychotherapy paradigm triumphed because it seemed to offer physicians a sensible explanation of why patients somatize and how to treat them…[but] no therapy that forthrightly assumed the non-organic nature of the symptoms would be accepted by the patients.”
INTERLUDE
We’ve seen a number of symptoms already rise and fall in popularity, in what is essentially a form of social contagion. Shorter emphasizes the role of physicians as vectors, inadvertently teaching patients what symptoms will and won’t be taken seriously in a given era. But how does this process start? How do disease memes enter the pool?
You may have noticed that psychosomatic entities have analogs in other medical conditions. There’s a form of the symptom that occurs “in nature,” which I’ll call the wild-type, and there’s a memetic form inspired by it. As Shorter says, “society does not invent symptoms; it retrieves them from the symptom pool.”
Wild-type form | Memetic form |
epileptic seizure | “hysterical fit” or convulsion |
nerve or spinal cord injury | limb weakness or numbness |
stroke | conversion blindness, speech impairment |
tetanus, dystonia | back arching, body spasms, ”drawing up” |
coma | trance |
sickness behavior (like flu) | chronic myalgia and fatigue |
heart attack | atypical chest pain |
In the wild-type form, the symptom is explicable as a malfunction in an identifiable biologic mechanism. By definition, this isn’t true of the psychosomatic, or memetic versions, which result from a still obscure central nervous system process.
We’re up to the 1920s - 1930s. Thanks to advancing science, doctors have more tools to discern non-organic illness. The psychological paradigm of somatization reigns in Western medicine. Where does this leave patients? ”Anxious to present legitimate disease, somatizing patients…abandoned the classic hysteria of the past and adopted sensory symptoms that would correspond to the new medical paradigms…pain and fatigue came to the forefront.”
Pain and fatigue have several useful qualities. They’re universal experiences with a range of causes. They’re poorly understood compared to seizures or focal paralysis. They’re inherently subjective and “almost impossible to disprove.” Thus, somatization in the rest of the 20th century consisted largely of patients reporting pains, fatigue, and other sensations like nausea or dizziness.
Profound asthenia of both physical and psychological nature at the end of the workday, a drop in attentiveness, in interest and in memory; disturbances of mood and personality, nervousness, irritability, episodes of anxious agitation, hypersensitivity to noise, hyperactivity with tearful moments
The pattern continued to the 1990s, when this book was written. The last few sections touch on Chronic Fatigue Syndrome (briefly attributed to chronic Epstein-Barr viral infection in the 1980s and christened “the Yuppie flu”) and Fibromyalgia. You can guess Shorter’s take: “From a grab-bag of scattered bodily pains, fibrositis (or fibromyalgia as some preferred to call it after muscle inflammation had failed to materialize) passed to being a specific disease.” With basically overlapping symptoms, he thinks Chronic Fatigue and Fibromyalgia are identical and probably represent a form of depression.
Shorter ends with pessimism. Loss of medical authority entails loss of control over illness attributions. Patients increasingly diagnose themselves with an assist from peer support groups and media-savvy charlatans. Ever-increasing social isolation, smaller families, and fewer intimate relationships make people unhappy and inwardly focused - fertile ground for somatization.
It is the lonely and disaffiliated who give us the image of our own times, who are the latter day equivalent of the hysterical nineteenth-century woman in her hoop skirts and fainting fits.
Did I mention this book was published in 1992?
From Paralysis to Fatigue has two major take-aways, and like any good history it raises intriguing questions about our own era.
First, the bodily symptoms that people describe change over time in a historically contingent way. Shorter’s symptom pool is a useful model, in addition to a forebear of predictive processing. Second, the rise and fall of these disease concepts is essentially a form of wide-scale social contagion. Somatization remains undoubtedly common, and waves of psychogenic motor symptoms are happening right now. While Shorter doesn’t use the term, I think memes are a good way to understand this.
But there’s no reason to restrict this model to physical symptoms. What happens once society adds a bunch of psychiatric disorders to the list of legitimate illnesses?
One version of this is fairly straightforward. Psychiatry goes through fads in diagnosis and treatment, and at least some psychiatric symptoms behave like a meme. The clearest example is Multiple Personality Disorder in the 1980s, and the contagious nature of self-harm behaviors and suicide has been recognized for decades. Eating disorders also seem to have a communicable quality. Ethan Watters’ Crazy Like Us (reviewed by Scott) provides memorable accounts of epidemic anorexia in 1990s Hong Kong as well as neurasthenia in Meiji-era Japan, proposing a prominent role for social contagion in mental illness.
This is all consistent with Shorter’s idea of the symptom pool. Once psychiatric symptoms are considered legitimate (or perhaps even trendy), more people have them. To be clear, just as with paralysis or fits, this isn’t intentional. In the examples above, the pattern is conspicuous because the symptoms were novel to the culture or the behavior itself was noteworthy.
A stronger version of this argument extends to more commonplace psychiatric conditions. Here’s how I would put it.
Just as with physical ailments, some people suffer from the wild-type form of a psychiatric condition. This includes psychosis and mania, and some forms of depression, and some panic attacks, and some OCD, and so on; these are ultimately due to a mechanism going awry in the person’s brain. There are also people who suffer with psychiatric symptoms that resemble the wild-type, but are actually the memetic version. These are ultimately due to the interaction of whichever illness memes are currently prevalent with a top-down “prediction” to experience those symptoms.
This distinction implies that some people experience prolonged sadness, or poor concentration, or panic attacks, or intrusive thoughts, but don’t have a “mechanism going awry” in their brain. Is this a coherent concept? If someone says they’re constantly sad, don’t they by definition have a mood disorder? If someone doesn’t eat and has a low BMI, don’t they have anorexia? By the DSM, yes. But we’ve just gone through a whole book about people who are in pain, or having seizures, or suddenly can’t talk, and we feel OK saying they don’t have an injury, or epilepsy, or a stroke.
If this hypothesis is true, you would expect to see shifts in how people experience common emotional symptoms, reflecting public awareness campaigns, media attention, drug marketing, and the cultural milieu. As far as I can tell, this is basically the consensus of historians in the field. It’s something like:
Anecdotally, I can tell you that bipolar disorder was very common from 2000-2012ish, but lately is surpassed by PTSD and ADHD.
Maybe people’s symptoms don’t change, but we just settle on new labels every 15 years, like a diagnosis treadmill? Maybe! I don’t think this is what historians would say. And if someone’s experience is so amorphous that they fit into bipolar disorder, depression, PTSD, ADHD, and anxiety…that’s kind of the point.
Maybe people had PTSD or depression or autism all along, and now we finally recognize it? Maybe! Though this reminds me of the Medieval Barber fallacy:
Theodoric of York: “You know, medicine is not an exact science, but we are learning all the time. Why, just fifty years ago, they thought a disease like your daughter’s was caused by demonic possession or witchcraft. But nowadays we know that Isabelle is suffering from an imbalance of bodily humors, perhaps caused by a toad or a small dwarf living in her stomach.”
Stigma about mental illness has certainly decreased over the years, which could account for overall higher rates of diagnosis and treatment than in the past. I don’t think it explains shifts in which symptoms people report and what they’re diagnosed with.
Why does this matter? One implication is that people coming to doctors and researchers with similar complaints have a mix of wild-type and memetic illness. The more attention a disorder receives, the greater the proportion of the memetic form. This makes for a confusing clinical picture since psychiatry lacks objective tests and relies, for most diagnoses, on what people say about themselves. High rates of memetic illness could also boost placebo response, with the effect that initially potent treatments like antidepressants and CBT appear to have lost effectiveness over time.
Is any of this plausible? I think the basic concept - that people can get “infected” with a psychiatric illness meme and develop a version of those symptoms - definitely occurs. Sometimes the memes are short-lived and dramatic, sometimes they’re so subtle and conventional that nobody realizes what happened until the history books are written.